Gender dysphoria (GD) is characterized by the incongruence between one’s experienced and expressed gender and assigned-sex-at-birth; it is associated with clinically significant distress. In recent years, the number of young patients diagnosed with GD has increased considerably. Recent studies reported that GD adolescents present behavioural and emotional problems and internalizing problems. Furthermore, this population shows a prevalence of psychiatric symptoms, like depression and anxiety. Several studies showed high rates of suicidal and non-suicidal self-injurious thoughts and behaviour in GD adolescents. To increase understanding of overall mental health status and potential risks of young people with GD, this systematic review focused on risk of suicide and self-harm gestures.
We followed the PRISMA 2020 statement, collecting empirical studies from four electronic databases, i.e., PubMed, Scopus, PsycINFO, and Web of Science.
Twenty-one studies on GD and gender nonconforming identity, suicidality, and self-harm in adolescents and young adults met inclusion criteria. Results showed that GD adolescents have more suicidal ideation, life-threatening behaviour, self-injurious thoughts or self-harm than their cisgender peers. Assessment methods were heterogeneous.
A standardised assessment is needed. Understanding the mental health status of transgender young people could help develop and provide effective clinical pathways and interventions.
Gender dysphoria (GD) is a condition characterized by a marked incongruence between one’s experienced and expressed gender and the one assigned at birth and is often associated with clinically significant distress or impairment in social, occupational, or other important areas of functioning, especially when reported early [1]. In recent years, the number of young patients diagnosed with GD or and gender-diverse identity—including nonbinary and questioning sexual identities—has considerably increased [2,3,4,5]. Current studies document that this population may be exposed to a higher risk of adverse events affecting health status and well-being [6, 7]. This further impacted this vulnerable population, with the most negative consequences for those who experience a gender not congruent with the one they were assigned at birth [8,9,10]. Indeed, children and adolescents with GD and transgender or transgender and gender nonconforming (TGNC) are described as a psychologically and socially vulnerable population, facing a wide range of physical and mental health concerns that could benefit from early intervention [11,12,13]. GD during adolescence develops in individuals whose brain is still developing to reach full maturity only some years later, hence the need to dedicate special attention to this population.
As a population perceiving gender minority stress [14], adolescents with GD are likely to lack social acceptance and suffer stigma laid upon them by others [15], but also tend to internalisation [16]. A corollary may be that several studies found adolescents with GD, compared to their age-matched cisgender peers, to show more often behavioural and emotional problems and higher levels of individual distress-generating internalising problems, rather than environment-perturbing externalising problems [17,18,19]. Consequently, adolescents with GD show a higher prevalence of psychiatric issues, such as depression and anxiety disorders [17, 20, 21], likely due to social stigma.
Adolescents and young adults with GD and gender-diverse identity report higher suicidal thinking, planning, and attempts as well as non-suicidal self-harming thoughts and behaviours (NSSI) than the general population [22,23,24,25,26,27,28,29,30,31,32]. Suicidality is an umbrella term including suicidal ideation, suicidal behaviours, and suicide attempts and plans which are correlated to the desire to die [33]; we will use suicidality sparingly in this paper and focus instead upon the above-mentioned specific terms, when possible. Non-suicidal self-harming behaviours and thoughts, however, refer to self-injurious acts without intending to end one’s own life, but involve self-punishment or negative emotion regulation [34]. In both cases, early age at onset has been identified as an important vulnerability factor, with onset during childhood and adolescence being associated with a poorer prognosis [17], based on different surveys of high-school students [31]. For example, in New Zealand, 20% of students with GD reported attempting suicide in the past 12 months, compared to 4% of all students [35]. Similarly, in the United States, 15% of students with GD reported a suicide attempt requiring medical treatment in the last 12 months, compared to 3% of all students [36,37,38]. In another American survey, 41% of students with GD reported having attempted suicide during their lifetime, compared to 14% of all students [39]. Moreover, Surace and her colleagues [40] found a mean prevalence of 28.2% for NSSI, 28.0% for suicidal ideation, and 14.8% for suicide attempts in young TGNC clinical populations up to 25 years old.
Besides aspects of GD like body dysmorphic disorder, feeling uncomfortable in one’s own body, and hopelessness about obtaining gender-affirming medical procedures, a possible contribution to elevated suicidal risk and behaviours in the GD population might lie within the social stigma experienced by TGNC adolescents, such as discrimination, prejudice, social stress, and ostracism within the peer group and/or family [41]. Suicidal ideation and self-injurious behaviours generally relate to significant emotional problems, such as depressive and anxiety symptoms, which in turn trigger psychosocial and biological imbalance, could increase the wish to die [42,43,44,45], thus adding to the above.
In summary, several studies have shown higher rates of suicidal and non-suicidal self-harming thoughts and behaviours in adolescents and young adults with GD and gender-diverse identity—such as nonbinary and questioning sexual identity—compared to their male and female cisgender peers. However, the evidence heretofore is piecemeal, probably due to social stigma currently associated with GD and the concern of stigmatising individuals suffering from this condition. To better understand the mental state of adolescents and young adults with TGNC, we conducted a systematic review focusing on the risk for suicide and self-harming gestures in the GD population. The aim of this review was to estimate the frequency of suicidal and self-harm behaviour in adolescents and young adults with GD, comparing them with cisgender adolescents where possible.
We performed a systematic review in compliance with the 2020 PRISMA guidelines for systematic reviews and meta-analyses [46] to increase comprehensiveness and transparency of reporting.
To systematically collect empirical studies on the possible relation between suicidality/self-harming and GD in adolescents and young adults, several keywords were used to search for appropriate publications in four electronic databases, i.e., PubMed, Scopus, PsycINFO, and Web of Science since their inception and no date or language restriction.
Authors conducted the search separately in each database using the following agreed upon search strategy for PubMed and adapting the search for the other databases: (suicid* OR self-injur* OR self-harm* OR self-inflict* OR self-lesion*) AND (gender dysphori* OR transgender) AND (child* OR adolesc* OR "young adult*" OR youth* OR "school age"). Since the terms GD and transgender are used by many people as synonymous, in our searches we used both terms to identify possible eligible articles.
Inclusion criteria were a study published in a peer-reviewed journal, reporting data on suicide and related behaviours (thinking, planning, and attempts) and/or non-suicidal self-harming thoughts and acts (using methods that reliably obtain the desired result) in adolescent and young adult (14–27 years old) samples with GD/transgender status/gender diverse identity.
Exclusion criteria were studies conducted on children or adult samples and those with mixed populations not providing data for adolescents and young adults separately. Also, opinion papers, such as editorials, letters to the editor, and hypotheses without providing data were excluded, as well as case reports or series, reviews/meta-analyses, animal studies, studies with inadequate/poor methodology and inadequate reporting of data, unfocused, or unrelated to the subject matter. All inter- and intra-database duplicates were removed, as well as abstracts, meeting presentations and studies presenting incomplete data.
Although reviews and meta-analyses were not included, their reference lists were screened to identify additional eligible publications. Eligibility for each study was decided with Delphi rounds among all authors until complete consensus was reached.
The analysis was conducted by all authors, who applied the eligibility criteria on each database. Each author conducted the selection process separately from others; at a final step, all authors compared their results in Delphi rounds (either in-person or remotely) aimed at obtaining full consensus.
Data collected for each study included country of origin, number of paediatric patients, demographic information (age and biological sex), presence/absence of GD and if present, type of GD, and clinical symptoms focused on self-harm (suicide behaviour, suicidal ideation, suicidal intent and planning, non-suicidal self-harm, and other self-injurious behaviour).
The evaluation of the risk of bias was conducted by a quality index derived from the Qualsyst’ Tool [47]. The quality of selected studies was assessed independently by all investigators and disagreements were resolved by consensus (results of risk-of-bias for all studies in the Additional file 1).
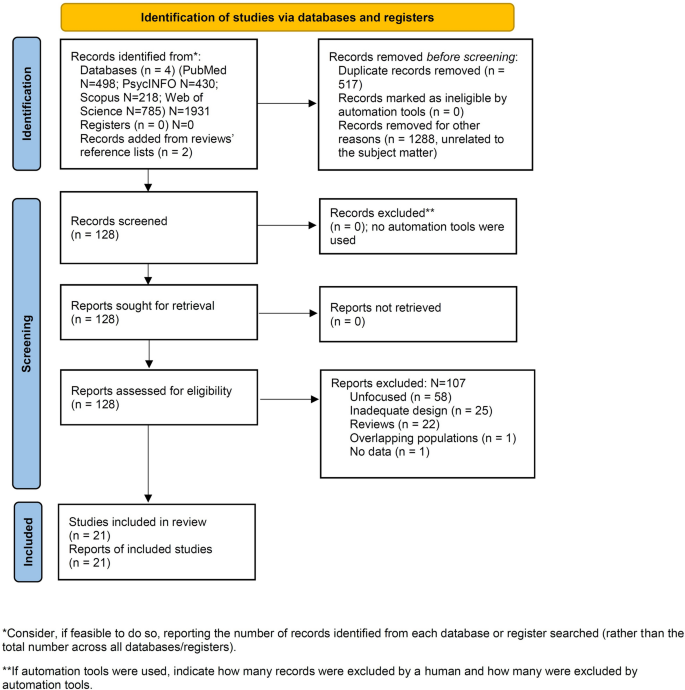
On February 7, 2023, we located 1416 articles (Fig. 1, PRISMA flowchart) [39], of which 128 articles were assessed for eligibility. Of these papers, 107 articles were excluded according to eligibility criteria; 21 dealing with the relationship between GD and gender non-conforming identity, and suicidality and self-harm in adolescents and young adults met inclusion criteria.
For the purpose of this systematic review, we have focused our analyses on these 21 studies. Figure 1 provides a PRISMA flow diagram showing search results.
Due to the breadth of the topic and the variety of variables included in this systematic review, the subject matter was organized according to the categories of psychopathological symptoms of interest in the study (Tables 1 and 2) and a final mixed category (Table 3). Of 21 studies meeting the inclusion criteria, there were 2 studies where self-harming behaviours and thoughts was the outcome in TGNC adolescents (Table 1), 6 studies where suicide was the outcome (Table 2), and 13 studies where the outcome was committing suicide combined to self-injurious attitudes (Table 3).
Table 1 Extracted data from included studies on gender dysphoria/transgender status and self-harming ideation/self-injurious behaviours
Table 2 Extracted data from included studies on gender dysphoria and suicidality (including suicidal ideation, suicide attempts and behaviours, suicide risk)
Table 3 Data extracted from included studies on gender dysphoria/TGNC/TNB, and both suicidality and self-harm
The 21 studies were mainly from the United States, the United Kingdom and Europe. Included studies were also conducted in China, Iran, Turkey, Canada and Australia. Studies were non-interventional and observational, with 17 being cross-sectional or retrospective and 4 longitudinal.
GD and non-suicidal self-harming ideation and behaviours were investigated by two studies [48, 49], GD and suicidality by six studies [6, 17, 24, 29, 39, 51], and GD and both suicidality and non-suicidal self-harm by 13 [11, 21, 22, 25, 30, 50, 52,53,54,55,56,57,58]; of these studies, four [11, 21, 55, 58] detected the presence of internalizing problems (depressive and anxiety disorders) in GD adolescents and young adults. Detailed results are provided in the Additional file 1.
Detailed results of each study are shown in Tables 1–3 and in the Additional file 1. We will here summarise results in GD and transgender populations regarding studies of (1) non-suicidal self-harm, (2) suicidal ideation and attempts, and (3) non-suicidal self-harm, suicidal ideation, and suicide attempts combined.
Additional considerations will be detailed further on.
The last decade has seen an increase in cases of GD in adolescents worldwide and our knowledge of the epidemiological and clinical features continues to evolve [59]. An adequate understanding of the phenomenon and any related symptoms is important for the early management and possible prevention of distress. Indeed, the literature has highlighted the existence of a high association of psychological and psychiatric symptoms in adolescents with GD.
Several studies used different methods to investigate whether transgender identity and clinical outcomes in the general adolescent population are related [6, 17, 21, 22, 24, 25, 29, 30, 39, 48,49,50,51,52,53,54,55,56,57,58]. The present review focused particularly on high-severity psychological symptoms in young people, such as self-harm and suicidal symptomatology. Indeed, the results of the studies underline a statistically significant correlation between youth TGNC—including gender dysphoric, non-binary and questioning adolescents—and prevalence of suicidal thinking and plans/attempts and self-harming thoughts and behaviours compared to cisgender populations [20, 29, 60,61,62,63,64,65]. Currently, there is a dearth of results from population-based samples, hence generalizing current findings is still very premature [59]. Despite progress and availability of resilience factors to face stigma and discrimination in some societies and social groups, there are considerable anti-LGBT attitudes in some countries and other social groups, ensuing in GD adolescents showing more mental symptoms and distress compared to cisgender peers [52, 66, 67]. Gender dysphoric adolescents show higher rates of depression leading to suicidal risk and engage in more self-injurious behaviours than their cisgender peers, confirming that a significant proportion of this population experience severe suicidal ideation and almost one third attempt suicide [4]. Other studies highlight that half of transgender youths are diagnosed with depression and anxiety disorders as well as poorer overall health and sleep quality [11, 66, 68]. Furthermore, puberty appears to exacerbate mental health problems in people with GD [30].
The main theoretical models, such as the gender minority stress model [69], identify potential risk factors among transgender individuals, link exposure to stigma, discrimination, and lack of social support. Previous research identified sexual minority status as a fundamental risk factor for own life-threatening behaviours [70]. In fact, adolescents diagnosed with GD experience victimization from their peers, negative parental reactions to their gender-nonconforming expression and identity, and family violence. These exogenous factors often lead transgender individuals to experience personal distress and isolation, which might elicit higher rates of own-life-threatening behaviours, such as suicidal attempts and ideation and self-harm thoughts than their heterosexual peers [70,71,72,73].
Overall, results of the studies included in this systematic review confirmed that, compared to cisgender adolescents, TGNC adolescents reported a significantly higher frequency of suicidal attempts, suicidal thoughts, making suicide plans, self-harm ideation and deliberately participating in self-harm acts. Higher depressive and anxiety symptoms and lower overall physical health were also positively associated with GD [11, 55, 57, 58, 74].
However, results were heterogeneous. Specifically, Wang and colleagues [11] indicated that among the gender minority groups transgender girls had the greater risk of planning and attempting suicide, transgender boys had the highest risk of performing deliberate self-harm, and questioning youth AFAB had the highest risk of suicidal ideation. Similar results were obtained in another study [24], with the risk ratios analysis highlighting the greater rate of suicidality among birth-assigned females. This pattern is consistent with many other studies showing that suicidality is more common among AFAB adolescents than it is among AMAB youth [75]. Some studies found possible gender differences between AFAB and AMAB and possible consequences for their mental health, suggesting that although AMAB might experience more stigmatization and preconceptions, AFAB youth seem to cope differently with distress [17, 25, 48]. Nevertheless, this outcome was different from Toomey and colleagues’ work [39], which found that transgender boys had a higher rate of attempted suicide than transgender girls.
At any rate, despite these within-group discrepancies, general findings emerging from quantitative studies provide evidence that a large proportion of adolescents referred for GD and other transgender youth, whether “AFAB” or “AMAB”, have a substantial co-occurring history of psychosocial and psychological vulnerability, causing a higher risk for suicidal ideation and life-threatening behaviours, such as self-harm thoughts and self-injurious gestures [70, 76].
Since society is becoming increasingly liquid according to Zygmunt Bauman [77], more cases of transgender states and GD are anticipated to occur; this will mean that we will have more of the general population at enhanced risk for self-harming acts, suicidal thinking, and suicidal behaviour. Under this perspective, it should be important to develop a comprehensive psychological assessment aimed at identifying people at risk of the above behaviours so to enforce preventive programmes [78,79,80].
For this reason, results provided by this systematic review may enhance the knowledge of health professionals about adolescents referred for GD. Furthermore, a better understanding of the mental health status of transgender youth and the associated risks could help to develop and provide effective interventions. The need for more knowledge and tools is also a key aspect of supporting each individual properly [30, 81]. Finally, increasing social awareness and scientific knowledge can also help target support programs for parents. Indeed, parents could benefit from interventions dedicated to understanding the impact of attitudes, behaviours and decisions, as well as assisting them in the therapeutic paths they take with their children with GD [70].
Limitations. This review contains heterogeneous data that could not be subjected to a meta-analysis. Heterogeneity regarded the instruments used to assess the populations included and the variables examined. To add to the high heterogeneity, the population under study belonged to multiple categories, such as cisgender males, cisgender females, individuals assigned female at birth whose experienced gender was male (so-called female-to-male transgender), individuals assigned male at birth whose experienced gender was female (so-called male-to-female transgender), and nonbinary. Often studies did not differentiate possible transgender from nonbinary identities. We attempted at focusing on GD only, but had to deal also with other populations as well, since the literature treats these populations as they were one and the same, which of course is not the case. Furthermore, a distinction between self-harm and suicide attempts was not always possible. Moreover, the social stigma laid upon gender diverse populations and current cultural trends may have directly or indirectly affected the writing of this review and its final results and conclusions.
In conclusion, the overall findings emerging from this review provide evidence that a large proportion of adolescents with GD have a substantial concomitant history of psychosocial and psychological vulnerability, with a higher risk of suicidal ideation, life-threatening behaviour, and self-injurious thoughts or self-harm. Understanding the mental health status of transgender young people could help developing and providing effective clinical pathways and interventions. The relatively new issue of suicide in adolescent/young adult populations currently suffers from poor assessment standardization. There is a need for standardized assessment, culturally adapted research, and destigmatisation of this socially vulnerable population to address the issue of increased suicidal thinking and attempts.